
BY ANISH KOKA
I just lately noticed a younger man who got here to see me as a result of his place of future employment, a big well being system was requiring him to finish the 1º collection of his COVID-19 vaccination. He was involved as a result of he had chest ache after his first mRNA vaccine and was uncomfortable with the dangers of a second mRNA dose. He tried to get a Johnson and Johnson vaccine and was advised by pharmacists he was not allowed to combine and match this specific vaccine as he had already acquired an mRNA dose. With no different choice, he got here to ask me whether or not I believed a vaccine exemption was cheap in his case. He already had a household drugs doctor signal an exemption that had been denied by his future employer’s vaccine exemption committee. The younger man works on the “again finish” of the well being system remotely from dwelling and he has no affected person contact. Your complete course of has precipitated him to lose his medical health insurance from his former employer, and he was now paying out of pocket for an costly COBRA medical health insurance plan. What follows is my letter to the vaccine exemption evaluate committee relating to his case. (Printed with permission, solely the related names have been modified/redacted)

Expensive Vaccine Exemption Evaluation Committee,
I’m penning this letter on behalf of John Smith DOB: xx/xx/xx in regard to a mandate from xxxx Well being that Mr. Smith obtain a second dose of an mRNA vaccine to finish his main COVID-19 vaccine collection.
Mr. Smith has requested me to render an opinion particularly associated to his cardiac threat of receiving a second dose of an mRNA vaccine. I’m a board-certified heart specialist in Philadelphia, Pennsylvania, and have been in lively medical observe for 13 years.
After reviewing the main points of his case, I’ve grave considerations about compelling him to obtain a second dose of an mRNA vaccine and wish to define the explanations for my conclusion on this letter. I’m going to particularly talk about his threat of an vital, now well-recognized, adversarial occasion: vaccine myocarditis.
What follows is a few vital background details about vaccine myocarditis that has been gleaned over the past 2 years earlier than I talk about the particulars of Mr. Smith’s case.
It’s related to notice right here that as a doctor lively clinically in each the inpatient and outpatient arenas, I’m an eyewitness to the extreme toll COVID-19 took on my sufferers within the Spring or 2020. I used to be impressed sufficient with the preliminary mRNA vaccine knowledge to amass the vaccine obtainable from the Philadelphia Division of Well being (Moderna) and ran a number of vaccine clinics with the intention to vaccinate my largely high-risk sufferers.
What follows is knowledge produced for the reason that vaccine rollout that’s related to Mr. Smith’s case.
The mRNA vaccines trigger myocarditis
The dangers of the novel mRNA vaccine had been first clarified in April 2021 by Israeli researchers who first recognized a causal hyperlink between the mRNA vaccines and myocarditis and likewise famous the upper incidence of myocarditis after the “second dose in younger males.”
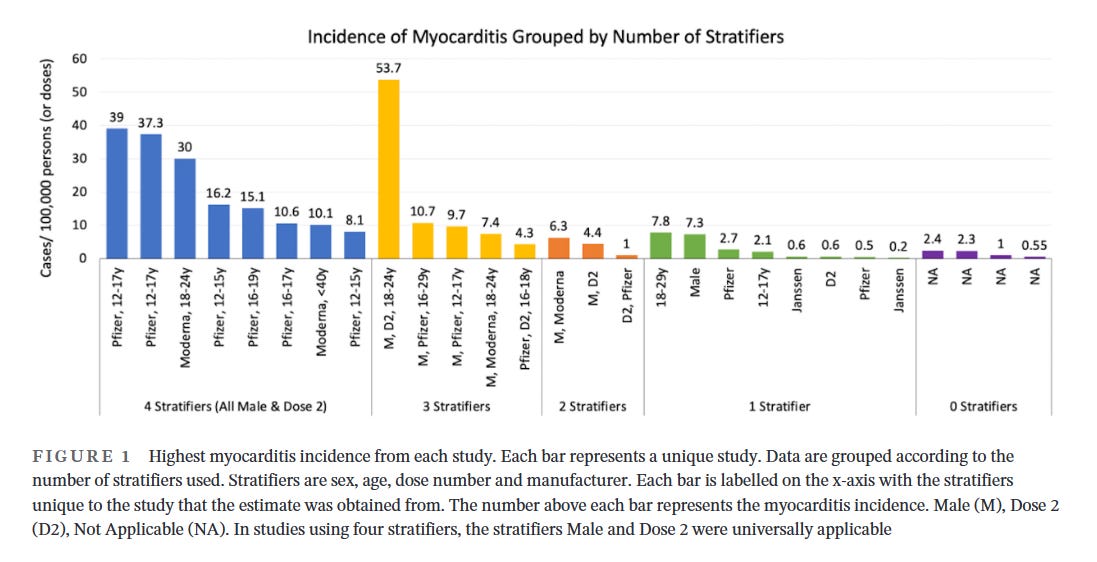
The very best incidence of vaccine myocarditis is in younger males after the second dose
Quite a few subsequent research which have tried to quantify the chance of myocarditis are of variable high quality largely as a result of a lot of research used pooled threat estimates throughout the complete inhabitants, ignoring the commentary that vaccine myocarditis has its highest incidence in younger males. Research that study the incidence of myocarditis by age, intercourse, dose and producer present essentially the most granularity with regard to threat estimation. A systematic review of vaccine myocarditis papers clearly demonstrates the best incidence of vaccine myocarditis in younger males after dose 2, and likewise highlights the uselessness of papers that don’t stratify incidence of myocarditis by age, intercourse and dose of vaccine.
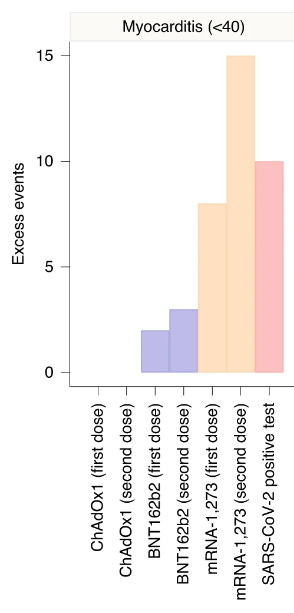
Vaccine myocarditis is larger threat than COVID myocarditis in younger males
A comprehensive study from England clearly demonstrated vaccine myocarditis to be extra frequent than COVID19 myocarditis in age < 40 regardless of the very fact this research tremendously overestimates COVID19 myocarditis charges as a result of it underestimates the overall variety of COVID19 infections.
Latest research carry into query the analysis of COVID19 myocarditis
A recent cardiac imaging study recommend myocarditis is just not the most important mechanism of cardiac damage after a COVID-19 an infection.
An accompanying editorial notes “Knowledge from COVID-Coronary heart present reassuring proof that myocarditis, as soon as predicted to be an rising public well being disaster attributable to COVID-19, is comparatively unusual even amongst hospitalized sufferers and is much less virulent than predicted in the course of the early days of the pandemic. It’s doubtless that elevated cardiac troponin concentrations throughout COVID-19 in lots of sufferers don’t replicate important new myocardial damage and fibrosis, however somewhat cardiac troponin launch from susceptible hearts with pre-existing scar within the setting of extreme sickness”
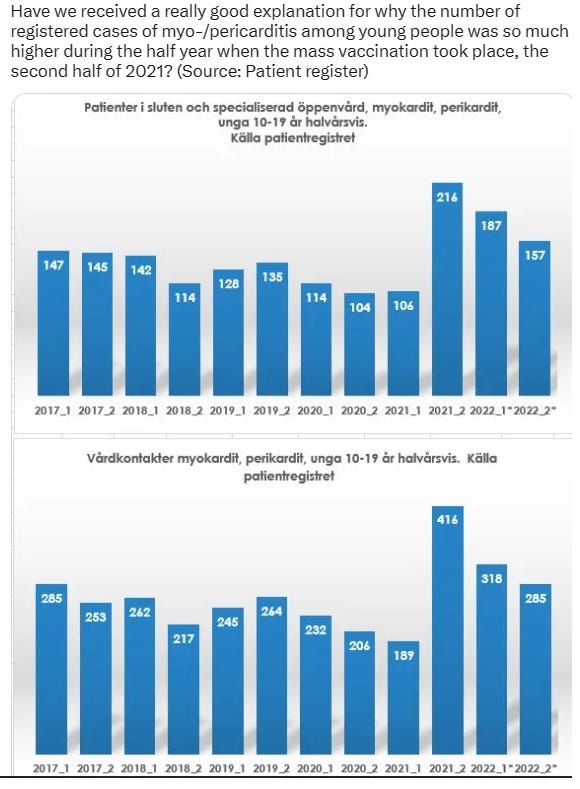
Knowledge obtained by a file request from Sweden clearly display elevated charges of myocarditis within the time interval after initiation of the COVID mass vaccination marketing campaign, with no considerable improve within the charge of myocarditis throughout widespread COVID within the yr prior.
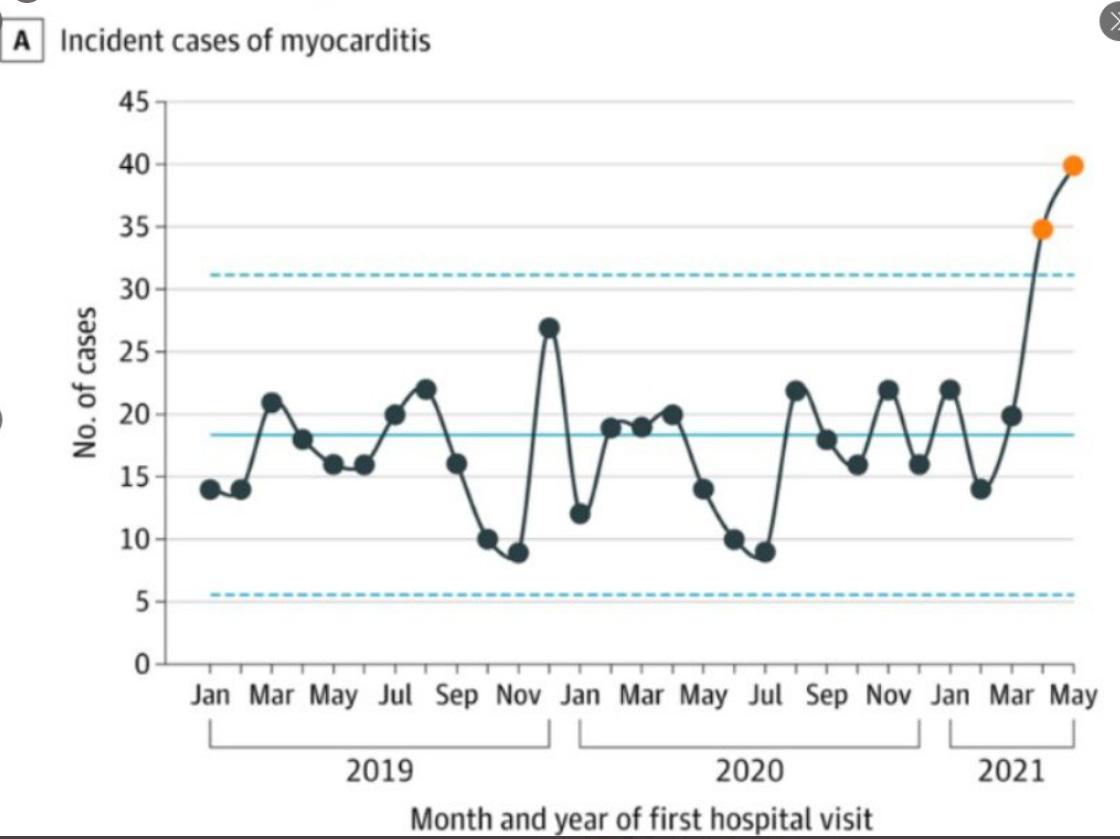
This spike in myocarditis diagnoses seen solely after initiation of the vaccination marketing campaign is corroborated by rigorous studies
6. requiring corroboration of a myocarditis analysis with the suitable medical context and cardiac imaging.
Restoration from a COVID an infection confers sturdy, sturdy safety in opposition to future COVID infections
A systematic review and meta-analysis of prior an infection with COVID suggests safety in opposition to re-infection “was very excessive and remained excessive even after 40 weeks.” The authors of this paper go on to recommend that “the immunity conferred by previous an infection needs to be weighed alongside safety from vaccination when assessing future illness burden from COVID-19”.
Vaccine myocarditis may be severe and life threatening.
The overwhelming majority of instances of vaccine myocarditis requires hospitalization for monitoring for deterioration. Whereas the vast majority of sufferers are discharged dwelling to recuperate, the present suggestion is for recovering sufferers to keep away from strenuous exercise for six months. A majority of sufferers that observe up for cardiac MRI imaging are seen to have scar in long run observe up. There are additionally case studies of extreme morbidity and mortality from vaccine myocarditis leading to important sickness or loss of life.
Prior episodes of vaccine myocarditis have been linked to an elevated threat of myocarditis with future vaccinations
Two case studies from Australia describe myocarditis after administration of the Novavax vaccine to 2 younger people who had recovered from mRNA vaccine myocarditis.
The 2 case studies from Australia aren’t even the primary studies of Novovax myocarditis after mRNA vaccine myocarditis. In August, the CDC reported 29 instances of pericarditis, together with 5 in individuals with a historical past of pericarditis after mRNA COVID-19 vaccine;
Importantly, the Novovax vaccine is a protein-based vaccine that was hoped to not be related to myocarditis as was famous with the mRNA vaccines. Sadly, these report of myocarditis occurring after Novovax supply in sufferers who had a previous case of mRNA vaccine myocarditis suggests a historical past of vaccine myocarditis ought to function a contraindication to any future COVID-19 vaccines.
Abstract / Suggestions:
Mr. Smith is a 31 yr outdated man with no medical historical past. He emphatically denies any historical past of cardiopulmonary illness. He acquired his first dose of a Pfizer mRNA COVID-19 vaccine in June 2021. He subsequently describes having sharp chest ache over the subsequent few weeks. He didn’t search any medical analysis on the time as he didn’t hyperlink the chest ache with the primary dose of the vaccine he acquired. The ache resolved a number of weeks later. He has had COVID twice, first in September of 2020, and his second time in January of 2023.
His cardiac testing accomplished so far encompass an electrocardiogram and an echocardiogram carried out Feb sixteenth, 2023 that had been each regular.
I feel it’s definitely potential Mr. Smith might have had myocarditis after the primary dose of his mRNA vaccine. As I mentioned with Mr. Smith, a cardiac MRI wouldn’t change my opinion on the matter as a standard outcome this many months from his unique presentation wouldn’t rule out acute myocarditis. If he did have a case of vaccine myocarditis after his first dose of an mRNA vaccine, I feel he can be in danger for creating myocarditis with one other COVID-19 vaccination. I’ll be aware right here that Mr. Smith did attempt to fulfill the mandate to finish a main collection of a COVID-19 vaccination by making an attempt to get a Johnson and Johnson vaccine. He was turned away by the pharmacists who famous the Johnson and Johnson vaccine was not accepted to be given after a primary dose of an mRNA vaccine.
As I’ve detailed, whereas most instances of vaccine myocarditis haven’t been proven to lead to extreme morbidity or mortality, there are clearly case studies of extreme vaccine myocarditis. Particularly given Mr. Smith has had two separate COVID infections, together with his most up-to-date an infection in January of 2023, it is extremely unlikely that the unclear advantages of a second dose of a COVID-19 vaccine are outweighed by the chance of vaccine myocarditis.
I perceive the committee has considerations past particular person safety almost about vaccination because it was hoped that vaccinations in opposition to COVID19 would scale back the probability of transmission of the virus and thus present safety to the group along with the person. As you recognize, the preliminary randomized management trials weren’t designed to check for discount in transmission, and the diploma of discount in transmission is a matter of debate now. Past the unknown efficacy of the vaccines associated to transmission threat, there does seem like rising consensus concerning the equivalence of a previous an infection from COVID and vaccination. The meta-analysis on prior an infection referenced above prompted the Chairman of Medication from UCSF, Dr. Bob Wachter to write :
Since practically all unvaxxed have been contaminated by now (many>as soon as), research lowers the case for vax mandates, since these w/ prior an infection doubtless have safety not materially worse than in the event that they had been vaxxed.
It must also be related that Mr. Smith is a non-clinical, distant employee who has no direct contact with sufferers or different healthcare workers.
For the entire above causes, I’d respectfully ask members of the vaccine exemption committee to rethink and grant Mr. Smith an exemption from the corporate’s vaccine mandate.
Yours Sincerely,
Anish Koka MD
Heart specialist
Philadelphia, Pennsylvania






{kind=link}