
Are non-English-speaking sufferers seen as shortly within the emergency division (ED) as English-speaking sufferers? If not, is that this hole restricted to sure non-English languages, or is it constant throughout all non-English languages? Is that this hole constant on weekdays? Is it extra pronounced on weekends?
It might be almost not possible for a medical or monetary operations workforce in your common emergency division (ED) to reply these questions shortly and precisely with out the precise knowledge. What’s extra, until a person has an analytical background, it might be extremely troublesome for them to know the place to start with knowledge exploration. But a lot of these questions are critically essential and related to understanding well being disparities and finally, well being fairness.
The COVID-19 pandemic surfaced longstanding social and racial inequities, and COVID’s disproportionate affect on folks from some racial and ethnic teams supplied a transparent instance of putting up with well being disparities throughout the nation. Efforts on the federal, state and native ranges are properly underway to start to mitigate these disparities, together with enhancing knowledge transparency and enhancing the fairness of care delivered all through the well being care continuum.
One instance of such an effort is on the Division of Emergency Medication on the College of Michigan Medical College, the place Dr. Christopher Fung, MD, led the development of an EHR-derived health equity dashboard to permit for the exploration of disparities in ED care. We lately spoke with Dr. Fung concerning the dashboard and the way improved entry to knowledge and metrics allows exploration and identification of well being disparities that will want additional investigation.
Solutions have been edited for readability.
Are you able to describe the intervention to create a dashboard on disparities within the ED?
As an analytics individual, I care about amassing the precise knowledge to be able to make data-informed selections. So usually, creating an information dashboard like that is useful for 2 issues: course of monitoring and knowledge exploration. With course of monitoring, we’re speaking about monitoring a selected course of over time utilizing a metric you already know very properly (i.e. the variety of sufferers seen per hour) whereas knowledge exploration is extra about asking questions of knowledge, normally with a speculation already partially fashioned or particular person observations that you just’d wish to discover additional. For instance, you would possibly query if there are variations in how shortly ache medicines are given to sufferers of a special race, or variations within the time it takes to see a health care provider relying in your race. With out one thing like a dashboard that lets you slice and cube knowledge, it is rather arduous to discover these well being disparities to appropriately problem a speculation. For this mission particularly, we leaned extra in the direction of the info exploration facet of issues however the dashboard is definitely helpful for course of monitoring too.
The benefit of working with ED knowledge, not like different components of the hospital apart from maybe the working room (OR), is that every one of our metrics are frequent and well-validated as a result of finally, EDs have to be as environment friendly as attainable. Most EDs within the nation are already meticulously monitoring issues like ready room time, how lengthy it takes for the physician to see a affected person, how lengthy it takes to get ache medicines and what number of CT scans or X-rays are ordered. Nonetheless, it’s uncommon that this knowledge is stratified by teams which have the potential to be marginalized of their care; for instance, race, ethnicity, sexual orientation, gender id, language, faith, age, and weight, amongst others. Moreover, it’s uncommon that such knowledge is accessible to these outdoors medical and monetary operations, comparable to resident physicians or different trainees.
What led you to tackle this effort? What function did resident physicians play on this mission and the way has it been useful for them?
Our goal with this mission was to develop an information dashboard that would supply resident physicians with prepared entry to ED knowledge to facilitate exploratory evaluation on disparities in ED affected person care as a part of an current high quality enchancment (QI) course of. Resident physicians in EDs throughout the nation play a crucial function in affected person care but a lot of them have restricted entry to related knowledge and restricted alternatives to have interaction in eliminating well being care disparities. Not solely is the required knowledge usually not obtainable to residents, however additionally it is arduous for them to know and work together with the info to get the outcomes they’re after.
The EHR-derived well being fairness dashboard, which went dwell in September 2021, is especially useful for residents as they work on the QI initiatives they’re tasked with to enhance well being fairness points. The dashboard offers a singular perspective enabling residents to visualise knowledge nonetheless they wish to uncover or discover disparities, start to know root causes, develop interventions and measure their affect.
Our preliminary imaginative and prescient was that everybody within the ED would have entry to this dashboard and particularly, resident physicians might work with their mentors on QI initiatives. The fact is that residents are extremely busy; a lot of them work 60-80 hours and whereas some are very research-driven and have interacted with the dashboard, the uptake has been slower than we anticipated. That mentioned, we simply rolled this out in September 2021 and new processes and workflows take time to rollout so we’ll see what the utilization seems like as we go ahead.
How is the dashboard being utilized by medical workers?
Lots of people are utilizing the dashboard however there are a number of superior views and buttons, which could be a little overwhelming. There’s a distinction between one thing printed for mass consumption, like what you would possibly discover on The New York Occasions’ “The Upshot” or FiveThirtyEight, the place it’s extra data-driven journalism with a easy visualization, than a sturdy knowledge dashboard like ours. As you begin including interactivity to a dashboard, it may possibly turn into an increasing number of overwhelming with each button you’ll be able to click on or possibility you’ll be able to change. In order that’s a problem for us to beat; getting customers of the dashboard to work together with it however not in a approach that’s overwhelming to them or confuses the image extra.
My basic sense is that individuals are rather more prepared to just accept knowledge journalism than they had been just some years in the past; each media group is doing that now. Most of the people is getting extra comfy with knowledge being introduced this fashion and the identical factor is going on in well being care with these types of dashboards and knowledge visualizations.
What classes have you ever discovered since implementing? Did you uncover one thing sudden?
Past the usability problem I described, I didn’t notice how troublesome it was for management to get data out of the Byzantine system that’s an digital medical document. Since placing the dashboard on the market, I’ve shortly realized how beforehand inaccessible this knowledge was. Earlier than I developed the dashboard, the outdated strategy to get that knowledge was to ship a bunch of emails that ultimately ended up with an analyst working static experiences. Now, it’s a lot simpler to ship somebody a hyperlink to the dashboard and so they can test for themselves.
Nonetheless, it will get just a little bit into the weeds once you add superior options like evaluating two teams in opposition to one another for some metric; that may turn into just a little overwhelming to of us. In order that’s kind of my ‘facet job’ as an information scientist; making the dashboard extra usable for folks different than simply myself.
What are your upcoming plans for the dashboard? What updates have you ever made to the dashboard? What’s the standing of among the ‘future instructions’ listed within the examine?
My main activity for this line of investigation is utilizing knowledge to drive a few of our DEI and fairness initiatives. Particularly, encouraging extra use of the dashboard amongst the trainees – each resident physicians and college students. They’re usually tasked with developing with well being care fairness QI initiatives and there’s a wealth of knowledge they will use to justify the mission they’re doing which is essential as a result of most initiatives require buy-in from nursing workers, administrative workers, and many others. Initiatives additionally requires cash, so it’s crucial to again up QI mission requests with arduous knowledge. I wish to make the trainees’ interactions with the dashboard – and knowledge basically – easy sufficient so that somebody with out an analytical background can do it. They want to have the ability to create the query after which go to the info for a extra in-depth evaluation to develop a rationale for his or her QI initiatives, or to give you new QI initiatives.
When it comes to future instructions, just about each ED within the nation has the sort of data already; these knowledge units we’re utilizing aren’t that unusual. They’re all dwell and so they’re all prepared for analytics; they only have to be overlaid with some components that may contribute to well being care inequalities like age, race, gender, and many others. So the long run effort is to scale; you’ll be able to scale throughout a bigger healthcare system and even unrelated EDs as a result of everybody has this knowledge already; you simply want the platform to place it collectively in a dashboard.
What different well being fairness work are you endeavor or planning to undertake? How can well being IT gasoline these efforts?
One of many issues I’m concerned about exploring is how the triage course of biases care within the ED. Most individuals don’t notice how influential these notes are; they closely affect how shortly you’re seen by a health care provider. Oftentimes that piece of documentation is the one piece that’s accomplished in your first day on the hospital, so everyone seems to be studying this one triage observe when you find yourself within the ED. If that observe has inaccurate data or it’s biased, that impacts your care. For instance, in the event you present up on the ED in ache however you look high quality, the observe will replicate that and there could be an assumption that you just don’t have to be seen as urgently. Proper or mistaken, these statements or notes are biasing and so they affect extra than simply time; in addition they affect whether or not or not you get ache medicines, get a CT scan, and many others. So the language that we use in these notes is doubtlessly biasing and that’s the place I’m beginning a brand new line of analysis; dissecting the language we use in triage notes and the way that influences care down the highway. It’s doubtless we’re biasing care throughout language or race even when that’s not in any respect our intention; for instance, medical doctors have a tendency to explain females as “hysterical” and that has a biasing impact on what suppliers consider that affected person, earlier than they even go within the room and meet the affected person. One other facet is designing interventions to cut back that.
The function a dashboard might play in one thing like that’s working an algorithm that analyzes the textual content of the notes based mostly on a language disparity rating, to find out whether or not or not that language might end in disparities in care. One thing like this is able to be useful to nurses, suppliers and others to allow them to higher perceive how the language in notes could be biasing and finally, draw a clearer line between language and outcomes.
What’s one thing that we didn’t cowl about this mission that we must always have?
We’ve collected a number of data and have a dashboard however one thing that’s not highlighted within the article is basically the subsequent step with a mission like that is getting management buy-in. In the end, it’s actually troublesome for any mission to realize momentum with out management curiosity. I’m a college member at a big educational hospital with entry to all types of sources and individuals who may help me do issues; even then it is rather, very difficult to show an enormous ship until the captain of the ship is purchased in to the place you have to go.
To study extra about ONC’s work to embrace well being fairness by design, go to HealthIT.gov. To study extra concerning the College of Michigan’s well being fairness dashboard, read the study.
Determine C: Time to first ache treatment by race. Mostly administered ache medicines had been recognized a precedence. Documented administration time is plotted as a survival curve the place administration of ache treatment is the occasion of curiosity. Decrease curves point out greater chance of receiving ache treatment.
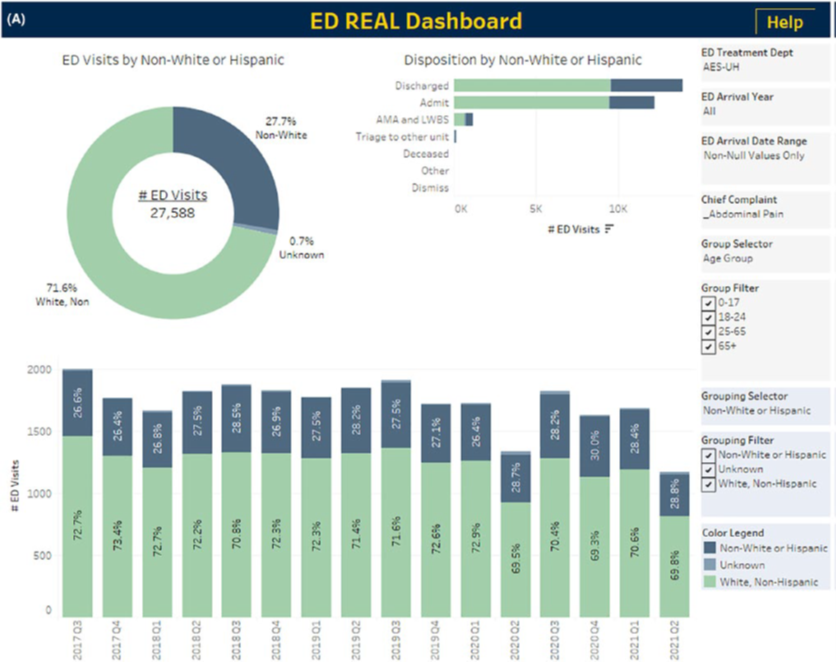
Determine A: Instance exploratory analyses utilizing the dashboard for first ache treatment by race and ethnicity in sufferers presenting with belly ache. REAL, Race, Ethnicity, and Language. All panels are filtered to grownup ED visits for belly ache and stratified by the next teams: White and non-Hispanic, non-White or Hispanic, and unknown race/ethnicity. Different selectable filters are on the proper of every panel. (A) Whole and quarterly distribution of ED visits by race with disposition. Counts and percentages are displayed for every of complete visits, quarterly visits, and inclinations.





{kind=link}